Works Cited
Alzheimers Association. http://www.alz.org/alzheimers_disease_what_is_alzheimers.asp.
5 May 2014. 2014.
Baudrillard, Jean. Simulacra and Simulation.
Michigan: The University of Michigan Press, 1994.
Callone, Patricia R. Alzheimer's disease: the
dignity within: A handbook for care givers, family and friends. New York:
Demos Medical Pub, 2006.
Descartes, Rene. "First meditation and excerpt
from sixth meditation." The Philosophical Works of Decartes Vol.1.
Cambridge: Cambridge University Press, 1967. 17-20. PDF.
Doka, Kennith J. Clinical Dimensions of
Anticipatory Mourning. Champaign: Research Press, n.d.
Long, Ph. D Janie. The Aging Family. New York:
BRUNNER/MAZEL, INC., 1997.
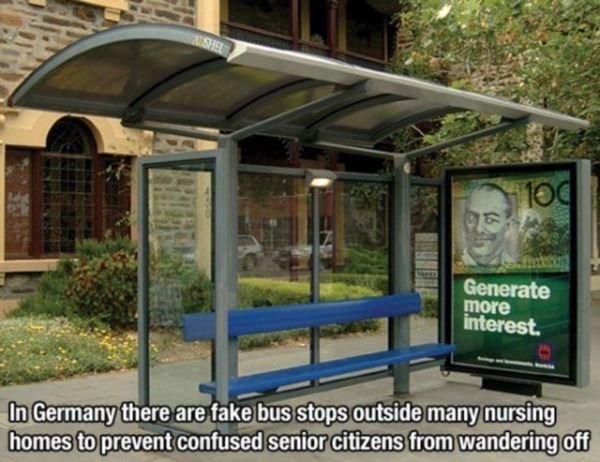
Lu Lu Miller. "The Bus Stop." Radio Lab.
n.d.
Saussure, Ferdinand de. http://faculty.smu.edu/nschwart/seminar/Saussure.htm.
n.d. may 2014.